

Sickle cell disease is a multisystem disorder associated with severe complications and premature death. To address the morbidity, disability, and mortality of inherited disorders, the implementation of newborn screening programmes are considered pivotal public health service intervention. Due to ethical consideration there are no RCTs that prove the benefits of comprehensive newborn screening (Lees, Davies and Dezateux, 2000). However, many evidences suggested early diagnosis and treatment can improve outcomes and survival of patients (Gaston et al., 1986; King et al., 2007). As such, an economic analysis reviewed many studies, cited that the pre-clinical diagnosis of SCD had twofold cost-effectiveness compared to symptomatic diagnosis (Grosse, Olney and Baily, 2005). The aim of this study was to assess the impact of the newborn screening program on the morbidity and mortality of disease among the children by assembling results from cohort studies.
DESIGN AND METHODS
The systematic review was performed in accordance with the PRISMA guidelines. Medline, EMBASE, and Cochrane Library were searched for cohort studies that addressed the sickle cell disease morbidity and mortality of the disease among children will consider eligible. The phenomena of interest were mortality, infection, stroke PICO have been translated to keywords and MeSH terms with search limit under 18 years old and date set until July 2020. Two reviewers assessed the quality of included cohort studies individually using Newcastle-Ottawa scale (NOS). Subsequently, the data were extracted in Microsoft Word. In case of disagreement, were settled by discussion. The incidence rates per 100 patient year and 95% confidence intervals were pooled to random-effects meta-analysis using RevMan5.4. Studies' heterogeneity identified by chi-squared test and the I2 statistic.
RESULTS
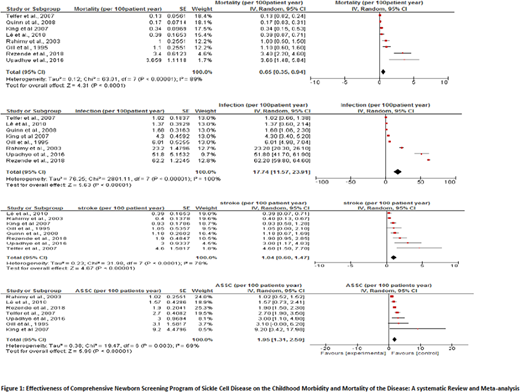
Eight studies included that met inclusion criteria two studies were from USA (Quinn et al., 2008 and Gill et al., 1995) , 1 from UK (Telfer et al., 2007), 1 from Belgium(Lê et al., 2010), 1 from Jamaica (King et al 2007), 1 from Africa (Rahimy et al, 2003), 1 from India (Upadhye et al., 2016) and 1 from Brazil (Rezende et al., 2018). The total number of participants in the 8 cohort studies were 2377 SCD patients (mean 297.1 and SE 73.9), that includes patients with the four common SCD genotypes: HbSS, HbSC, Hb Sβ+ and HbSβ0. The median age was 6.5 year (IQR: 4.95), with 9623 total years of follow up. The pooled incidence rate of SCD associated mortality per 100 patient year was 0.65 (95%CI 0.35-0.94; I2= 89%; p < 0.00001). While the infection incidence rate 17.74 (95%CI; 11.57-23.91; I2= 100%; p< 0.00001), Stroke 1.04(95% CI 0.60-1.47; I2= 78%; p< 0.0001), Acute chest syndrome 12.55(95% CI; 7.70-17.41; I2 =97%; p< 0.00001), Acute splenic sequestration crisis 1.95 (95% CI 1.31-2.59; I2= 69%; p=0.003) and Vaso-occlusive crisis 52.45(95% CI 45.67-59.14; I2= 92%; p< 0.00001).
DISCUSSION
In this systematic review and meta-analysis combining 8 cohort studies, pooled mortality rate was 0.65 per 100 patient-year, similar to (0.64) meta-analysis of 15 studies reported previously (Wastnedge, 2018). Furthermore, our study reported that the total infection rate was 17.7 per 100 patient-year. However, this result of infection cannot be considered a true gold standard and due to the variation in definitions used and other methodological heterogeneity. For example, Africa-based cohort study reported 23.2 per 100 patient-year attacks of malaria and fatal pneumococcal meningitis despite the use of antimalarial prophylaxis and anti-pneumococcal vaccine (Rahimy et al., 2003). Another notable result, Hemoglobin SC cohort study stated that the incidence of infections was, 62.2 episodes (59.8-64.6) per 100 patient-years. They assumed that might be due to higher impaired splenic function in HbSC patients compared to HbSS (Rezende et al., 2018).
CONCLUSION
This first systematic review and meta-analysis of cohort studies provided evidence supporting the sickle cell newborn screening program. However, still infection and pain episodes are the highest incidence symptoms. Despite children survival increasingly improved, disease burden remains at a peak in developing countries. One limitation of this study is high heterogeneity and this mainly due to countries disparity of included studies and variance in definition of events, particularly infection.
Inusa:Novartis: Honoraria, Other: Steering committee participation, Research Funding, Speakers Bureau; Global Blood Therapeutics: Honoraria, Other: Steering committee participation, Research Funding, Speakers Bureau; Bluebird bio: Research Funding; AstraZeneca: Honoraria, Other: Steering committee participation, Research Funding, Speakers Bureau; Vertex: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal